Multifocal motor neuropathy (MMN) with conduction block is an acquired immune-mediated demyelinating neuropathy, which causes slowly progressive weakness, fasciculations, and cramping. It can resemble amyotrophic lateral sclerosis (ALS) with predominant lower motor neuron involvement, but distinction is important since MMN usually improves with immunosuppressive treatment.
MMN is more common in men than women with a mean age at onset of 40 years (range of 20–70). The most common initial symptoms are wrist drop, grip weakness, and foot drop. Weakness progresses asymmetrically, but usually remains more prominent in the arms than in the legs. Weakness is typically more pronounced than would be suggested by the degree of muscle atrophy present. Affected patients also complain of muscle cramps and fasciculations. Tendon reflexes are reduced in affected regions. Sensory complaints are unusual.
These symptoms and signs from MMN are very similar to those seen in early ALS, and many patients are initially misdiagnosed with this disorder. MMN can usually be distinguished from ALS by its more slowly progressive disease course, the absence of upper-motor-neuron signs such as spasticity and hyperreflexia and the lack of difficulty with speech and swallowing.
However a carefully planned and executed electrodiagnostic study (EMG) is critical for distinguishing these disorders. MMN is a demyelinating neuropathy, while ALS is an anterior horn cell (motor neuronopathy) which causes secondary axonal degeneration of the motor nerve. When one suspects MMN clinically, identifying partial motor conduction block is critical in confirming the diagnosis.
The presence of high titers of antibodies to GM1 ganglioside can also be useful for confirming the diagnosis of MMN, but are only present in 20-60% of patients, and are rarely present in ALS patients, underscoring the importance of clinical suspicion and the EMG for making the diagnosis.
MMN is an immune mediated disorder and strength can recover after repeated treatments with intravenous immunoglobulin (IVIG), whereas ALS does not respond to this or any other treatment, hence the importance of distinguishing these 2 disorders:
Disease MMN ALS
Distribution of weakness Asymmetric,Arms Ultimately generalized
Upper motor neuron findings Absent Usually present
EMG Conduction block Motor axonal loss
Anti GM1 Ab 20-60% 10%
Response to IVIG Yes No
The clinical pictures below are from a patient with longstanding generalized weakness that I encountered several years ago. The first picture shows his severe upper limb atrophy (and weakness):

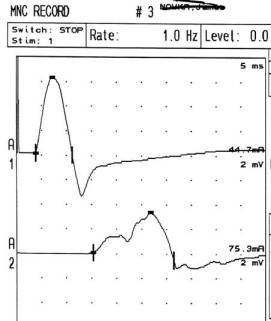
His EMG showed conduction block, suggesting MMN:
And the second picture showed the clinical improvement that had already occurred after 6 monthly treatments with IVIG:

Obviously it is important to at least consider this treatable disorder in all patients with suspected ALS or motor neuron disease, and it is very important to see a neurology specialist with additional training and certification in neuromuscular medicine and/or electrodiagnostic medicine. Click here or call 732 923-5576 to find out more about the Central Jersey MDA and Neuromuscular Center at the Monmouth Neuroscience Institute.

Hi and thank you for your help.
I have been diagnoses with MMN a year and a half ago. I did receive Gammagard IVIG since then. At the beginning once every month then once every 3 weeks, now every 2 weeks. I have fasciculation ( a lot ) in my right shoulder and right arm, atrophy right hand, i can still use it but unable to write anymore. I started fasciculation in my right thiht. Last week they suggested we try Rituximab as a complement. To me it is obvious IVIG have not stopped degradation although i feel a lot better now than i receive them every 15 days and i see when It comes to the last days that weakness increases. My worse symptoms are weakness and fasciculation.
Would you suggest Rituximab ? And what are the side effect ?
Is there another treatmennt possible ?
What to think about celltransplant ?
Onve again thak you for. Your Answer. It is appreciated.
Thanks for your comment. Obviously it’s really hard to comment without knowing the details of your case. I have had patients who need IVIG every 2 weeks. However, if you feel like you are not improving or getting worse despite that, you might want to get another opinion before trying rituxan.
hi, can you tell me if it is advisable to stop iv IG TREATMENT being done 6 weekly on a pregnant 33 yr old who has had MMN for 10 years. she is 7 weeks pregnant and has been told that it is not advisable to continue the treatment while pregnant.
will her symptoms not worsen? and will they improve once pregnancy finished
That’s a great question. Administering medications to pregnant women is always a complicated and emotive topic. Many women prefer not to take any medications at all while pregnant. MMN patients who miss IVIG infusions (for whatever reason) will get worse, but will usually get better again (although sometimes slowly) once the treatment is re-started. We frequently encounter MMN patients who gone undiagnosed and untreated for many years (like the patient described here) who still improve with IVIG. Auto-immune diseases tend to be less intense during pregnancy in general. However, if the MMN were to get really severe and disabling with 9-months missed treatment, it could affect the woman’s ability to take care of (and bond with) the baby in the immediate post-partum period. Furthermore, there is increasing data that IVIG can be safely administered throughout pregnancy – it has been used in lupus patients with antiphospholipid antibodies to prevent abortions, and has also been given to pregnant MS and myasthenic patients to prevent relapses. In sum, I think whether to continue or stop the IVIG during pregnancy is a complicated decision that would depend on the opinions of the neurologist, the obstetrician and the severity of the MMN.
Thank you much for your help, I will try to get in touch with dr Hahn. London is not that far from where I live.
Do you know a medecine that can stop fasciculations caused by MMNBC ? I have them in right shoulder right arm /hand and just started to have somein my right leg and now left arm.
Thanks again
Probably nothing, aside from treating the underlying disease. Sometimes drugs like gabapentin or carbamazepine are helpful for cramping.
thanks a lot for these answers
I am affected with MNNBC and I wonder who would be THE specialist in Canada, if you have an idea ?
I am sure there are many wonderful neurology and neuromuscular programs in Canada that I am simply not aware of. I do know there is a very good neuromuscular program in London, and Dr Angelika Hahn has published papers and presented data at national meetings on immune mediated neuropathies including MMN.