Post prepared by Precious Ramirez-Arao, Monmouth Medical Center PGY3
A 60 year-old female was found lethargic lying in a pool of feces by roommate.
EMS was called and was immediately brought to the hospital.
In the emergency department she had a witnessed generalized tonic-clonic seizure.
Her roommate relates she had episodes of confusion and short-term memory loss over the past few weeks.
She remained lethargic over the next 72 hours in the hospital.
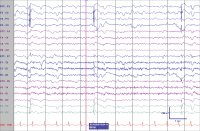
48-hour EEG monitoring showed diffuse 2 to 3 Hz delta slowing with periodic lateralized epileptiform discharges emanating from the left frontal temporal region.
T2 weighted image of the brain showed signal abnormality of the left mesial temporal lobe and the pulvinar with diffusion restriction in the left hippocampus consistent with limbic encephalitis.
Limbic encephalitis (LE) is a subacute syndrome of seizures, personality change and cognitive dysfunction, typically evolving over days to weeks.
Autoimmune and paraneoplastic forms have been described. The most common neoplasms associated with paraneoplastic LE are lung cancer (usually small cell), thymoma, ovarian or testicular teratoma, breast cancer and Hodgkin lymphoma. The associated autoantibody depends on the tumor type. Lung cancer and thymomas are associated with anti-VGKC while ovarian or testicular teratomas are associated with antiNMDA antibodies.
Neurologic symptoms can precede oncologic diagnosis for several months to years and initial CT scans are typically unrevealing.
Nevertheless, prompt and thorough evaluation for malignancy including PET and CT scan of the chest, abdomen and pelvis should be initiated. Symptomatic treatment includes corticosteroids, plasmapharesis and intravenous immune globulin.
Here’s an illustrative example from a conversation with FD, an elderly woman who had had a right hemispheric stroke one week before, leaving her paralyzed on the left side and confined to a wheelchair:
How are you feeling today?
FD: I’ve got a headache. You know, doctor, I’ve had a stroke so they brought me to the hospital.
Can you walk?
FD: Yes (FD had been in a wheelchair for the past week, and cannot walk)
Mrs D, hold out your hands. Can you move your hands?
FD: Yes
Can you use your right hand?
FD: Yes
Can you use your left hand?
FD: Yes
Are both hands equally strong?
FD: Yes, of course they are equally strong.
Mrs D, point to me with your left hand.
FD: (Her hand lays paralyzed in front of her).
Mrs D, are you pointing to my nose?
FD: Yes
Can you see it pointing?
FD: Yes, it is about 2 inches from your nose.
Mrs D, can you clap?
FD: Yes, of course I can clap.
Mrs D, will you clap for me?
FD: (She proceeded to make clapping movements with her right hand, as if clapping with an imaginary hand near the midline)
Are you clapping?
FD: Yes, I am clapping.
xx
xx
The term anosagnosia was first used by Joseph Babinksi on June 11, 1914 in a brief communication presented to the Neurological Society of Paris.
He described two patients with left hemiplegia who didn’t know they were paralyzed. The word comes from the Greek words nosos, “disease”, and gnosis, “knowledge”.
Affected patients deny their deficit, and overestimate their abilities, they state that they are capable of moving their paralyzed limb and that they are not different than normal people.
Their false belief of normality persists despite logical arguments and contradictory evidence – they may even produce bizarre explanations to defend their convictions.
If they admit any impairments, they will attribute them to other causes (i.e. arthritis, tiredness, etc.).
xx
xx
But, this syndrome is not only seen with hemiplegia.
Visual anosognosia or Anton-Babinski syndrome is a rare neurological condition related to cortical blindness. Affected patients deny their blindness and affirm adamantly that they are capable of seeing. The clinical presentation includes confabulations – instead of admitting blindness, they will make up answers when asked about what they see.
Mr Magoo is a great TV example of Anton’s syndrome – unaware of his loss of vision, he misinterprets and confabulates his way into trouble.
xx
Anosognosia may occur as part of receptive or Wernicke’s aphasia – affected patients cannot monitor and correct their own speech errors and may appear angry and frustrated when the person they are speaking to fails to understand them.
xx
Watch this lecture, by Dr V. S. Ramachandran for more information on this fascinating syndrome:
Methamphetamine was legally prescribed in injectable form in the US in the 1930-50s as a central nervous stimulant, antidepressant and appetite suppressant (for weight loss).
It became a widely abused prescription drug in the 1960’s, before it became more tightly regulated by the government in the 1970s.
That is when illegal manufacturing and distribution really started to take off in the US.
In the 1980s a new crystalline form of methamphetamine, which could be smoked, found it’s way into the US, and quickly started to replace cocaine as the illicit stimulant of choice among drug users.
Whether snorted, smoked, or injected, methamphetamine rapidly crosses the blood brain barrier where they cause sustained increases in the extracellular concentrations of monoamine neurotransmitters such as dopamine, norepinephrine, and serotonin.
With repeated use in both humans and experimental animal models, methamphetamine depletes the brain’s stores of monoamines, contributing to methamphetamine’s high abuse potential – without the drug, users may have an impaired ability to experience pleasure (anhedonia), slipping into a deep depression
Dopamine and serotonin neurons project widely throughout the brain influence a variety of behaviors and functions. Up to 40% of chronic methamphetamine users have memory loss, impulsive behavior and impaired decision-making. Continued drug abuse can lead to depression and psychosis.
One interesting aspect of chronic methamphetamine psychosis is the delusion of parasitosis or formication – commonly known as “meth mites”, this is a frequent complaint in heavy daily users of methamphetamine, and can lead to self mutilation:
Bovine spongiform encephalopathy also known as “mad cow disease”, is another prion disease that affects cattle, and was responsible for bringing more attention to all of these disorders in the 1990s.
Kuru is confined the Fore tribes of Papua, New Guinea.
In the 1950s there were 2100 cases of Kuru in these tribes leading to about 1000 deaths per year.
As per the culture of the Fore tribe, if a person in a family dies his meat is eaten by his family members, especially the wife and children, as a mark of respect to him. 90% of people affected by the disease were women and children.
Between 1996 to 2004 only 11 new cases of Kuru were identified in the region. Currently with the ban of cannibalism in the Farah tribes the disease had become virtually non existent.
Kuru first presents with tremors, then unsteady gait and progresses to leg weakness, ataxia, incoherent speech, sporadic laughter finally. In later stages, affected patients become demented, bed bound and unable to swallow.
Death occurs most commonly from respiratory distress and pneumonia or infection of pressure sores. The disease is fatal within 1-2 years of the onset of symptoms and had no known cure.
Here’s a video introduction
Watch the full story here:
The causative organism is a prion, a mutated protein which replicates itself like a virus, and is spread by eating the neuronal tissue of infected people.
The precise incubation period of the disease is unknown, but can be up to fifty years.
The pathological hallmark is the presence spongioform encephalopathy with of Prion reactive plaques mostly in the cerebellum:
The detailed studies of theses cases of Kuru has helped us understand other prion diseases such as variant CJD, sporadic CJD whose clinical features and course is similar to this condition.
Posted by Sanya Naware MSIV, Drexel University College of Medicine
What would it feel like to only perceive one half of the world around you?
For patients with hemispatial neglect, this is an everyday reality. Hemispatial neglect or hemineglect is a condition in which damage to one hemisphere of the brain causes a lack of awareness of one contralateral side of space. It is most often a lesion of the right posterior parietal cortex affecting the contralateral side of the body. The person is unable to recognize stimuli or process them on the affected side. Left neglect is more common than right neglect because the right hemisphere is able to compensate for the loss of left hemispheric function.
Because these patients only perceive one side, they only draw what we know to be half of an image as seen in the video and image below:
Lisa Genova, a neuroscientist, expertly describes the daily challenges of living with neglect in her book Left Neglected. It is a difficult condition to imagine and this book does a wonderful job of explaining the realities and frustrations of the patient and her family.
The main character, Sarah Nickerson, suffers a traumatic brain injury in a car crash. When she wakes up, everyone around her realizes that she ignores the left side of everything. Whether it is a clock, a painting, or a room around her, she is not able to recognize the left side of anything. While she is able to feel the left side of her body, she has to focus on the fact that she has a left side in order to control her left leg and walk. In fact, when she first sees her left arm, she states that it feels like it belongs to another person, a problem called somatoparaphrenia. While eating, she only eats the food on the right side of her tray. She frequently bumps into objects on the left side of her body because she is unaware of their presence.
Sarah’s story is optimistic as her therapist and family use certain tricks to help her adjust. Some of these methods include placing bright orange tape on the left side of things around their home, using a ruler to guide her to the left side of the page, and wearing shiny jewelry on her left hand to attract attention to it.
Everybody knows October is the month of horror movies, haunted houses and Halloween parades.
But, have you ever wondered why we find fear so exciting?
It turns out that distress and delight are closely related – both are mediated by same deep brain circuit known as the Limbic System. This system is intimately associated with human emotional behaviors and memory.
The limbic system is highly interconnected with the brain’s pleasure center, responsible for sexual arousal and the “high” derived from recreational drug use, The Kluver-Bucy Syndrome, caused by bilateral limbic lesioning, includes heightened sex drive and/or a tendency to seek sexual stimulation from unusual or inappropriate objects.
Animals with surgical lesions to the limbic system develop abnormal sexual behaviors
Recent studies have shown these same circuits are responsible for associating fear with memories and the emotional responses that result from triggering those memories. Patients affected by the extremely rare genetic condition Urbach-Wiethe disease can develop selective atrophy of the amygdala, becoming fearless, with little or no emotional response to horror films, large spiders or snakes.
This probably explains why horror movies are most popular with younger audiences, mostly teens and twenty-somethings with raging hormones looking for intense experiences:
xx
So, we go to horror movies to be scared, triggering deep seated pleasure centers within the brain, knowing that we’re actually quite safe from harm, because in an hour or two we’re going to walk out of the theater with no permanent harm done.
Posted by Deepak H. Singh, MS IV Drexel University College of Medicine
Putting my intense desire to describe the mauve affect of a patient, or the loud shirt that a colleague is wearing aside, synesthesia is a fascinating phenomenon in which two or more senses in certain individuals are overlapped, meaning that the experience of both senses is connected in someway.
This has been described in terms of various different senses including forms such as grapheme-color synesthesia in which letters and numbers are perceived as colors, chromesthesia in which sounds are perceived as color, or lexical-gustatory synesthesia in which individual words are perceived as taste sensations in the mouth as alluded to in the title of this blog post.
Click here to find out more about word-taste synesthesia from the BBC.
This condition has long perplexed neuroscientists who are only touching the surface of the unique neural pathways that may account for the various experiences described by synesthetes.
One school of thought that has gained some traction is the concept of cross-activation, which is made possible by a failure of the physiological process of “synaptic pruning” that occurs in all of our brains during the initial developmental stages. Synaptic pruning refers to a series of regulatory processes during which various axonal networks that were functional in one stage of development are outcompeted and subsequently eliminated as other synaptic connections become more frequently used as maturation occurs. In synesthetes it is hypothesized that certain of these connections fail to regress leading to atypical connections between two sensory regions of the brain, thereby opening the door for some pretty vivid sensorial experiences. This, however, has only really held up for sensory regions directly adjacent to one another, as was demonstrated by fMRI studies showing significant brain activity in both the auditory cortex and the fusiform gyrus (responsible for color perception) in synesthetes while no such congruous activity was seen in age-matched controls. Similarly, in one study on lexical-gustatory synesthesia, the lateral sulcus (responsible for taste processing) was activated simultaneously with the auditory cortex in synesthetes.
Another prevailing hypothesis is the concept of “disinhibited feedback“. Normally, signals are travelling in both directions between the primary sensory regions of the brain and those that are involved in organizing that information, and feedback (both positive and negative) is constantly occurring to reconcile all of the different sensory input. If this balance were disrupted, however, it would be possible for signals encountered in the later stage of processing to influence those that were encountered earlier, resulting in the overlapping sensations that are perceived by synesthetes. This, too, may make more sense of the case reports in which individuals with temporal lobe epilepsy or individuals who have just experienced head trauma or stroke to “acquire” a synesthesia-like experience due to some disruption in those pathways, though no concrete studies have been done to test that theory.
Perhaps we’ll never know what is truly occurring at a neuroanatomical level that causes such a curious phenotype. In the meantime, looking at the accomplished list of puported “sufferers” of this condition, it may be worthwhile to pose the following question: which came first the synesthesia or the visionary?
To fully understand Concussion’s Axis of Evil, one need look no further than the brutal world of professional boxing and it’s neurological complications.
xx
xx
xx
One of the most savage beatings any fighter every received occurred on July 4, 1919 in Toledo, Ohio, when 24 year old Jack Dempsey destroyed 37 year old Jess Willard to become the Heavyweight Champion of the World.
One can easily spot the effects of concussion in Willard as he sustains blow after blow to the head, and he develops unsteady gait, erratic behavior (failing to avoid punches and protect himself) and ultimately unconsciousness.
New Jersey’s own Harrison S. Martland MD (1883-1954) was the first to report in 1928 that repeated beatings of this kind could lead to a delayed permanent neurologic syndrome referred to as punch drunk syndrome.
xx
His observations went largely unheeded.
xx Muhammad Ali (born as Cassius Marcellus Clay in 1942) was only 22 when he became word heavyweight champion in 1964, almost 40 years after Martland’s paper was published.
Almost 10 years after that performance, Prof Corsellis reported further clinical and pathological features of punch drunk syndrome in his 1973 paper “The Aftermath of Boxing”.
Here’s data from one of his cases:
xx
Obviously, repeated head trauma, and it’s consequences, is not unique to boxing:
John Grimsley (1962-2008) was a linebacker for the Houston Oilers. He retired in 1993. In 2008, aged 45, he was killed by an accidental gun shout wound to the chest.
His brain showed the same pathologic changes as the Punch Drunk boxers.
xx
xx
xx
xx
xx
xx
This syndrome, more commonly referred to as Chronic Traumatic Encephalopathy, is now known to have occurred as a consequence of repeated head trauma in many other sports, including soccer, hockey, horse-racing and wrestling.
College football and amateur soccer players have been shown to have impaired performance on neuropsychologic testing, worse with increasing number of concussions.
SIS is said to be a rare, often fatal, traumatic brain injury that occurs when a repeat injury is sustained before symptoms of a previous head injury have resolved.
Although limited to single case reports, and disputed as a discrete syndrome in the scientific literature, SIS cases are young athletes and have become high profile in the media: Click here to find out more about this case.
It has become clear that it takes athletes longer to recover from repeated that single concussions:
This data, as well as SIS cases, has led to a concern that the presence of ongoing concussive symptoms are a significant risk factor for further injury to occur, and that any residual symptoms should mandate restriction for further contact sport in young athletes.
xx
xx
Finally, it is know that concussions are under-reported by high school players.
A 2004 survey of 1500 varsity football payers in Milwaukee disclosed that although 15% had sustained a concussion during the season only 50% reported it to their coach or trainer.
Post written by Dr. Hadi Razjouyan, PGY III Internal Medicine Resident at Monmouth Medical Center
Introduction
Serotonin syndrome is a rare and potentially life-threatening toxic state caused by excessive serotonergic activity in the nervous system.
It was first described in 1960s in studies of antidepressant medications and classically consists of a triad of mental status changes, abnormalities of muscle tone, and autonomic hyperactivity. However, clinical manifestations can be diverse and nonspecific, leading to misdiagnosis. Most reported cases are in patients using multiple serotonergic drugs, or who have had considerable exposure to a single serotonin-augmenting drug:
Medications that may contribute to serotonin syndrome. (Ables AZ, Nagubilli R. Prevention, recognition, and management of serotonin syndrome. Am Fam Physician. 2010 May 1; 81(9):1139-42).
Epidemiologic features
It can happen in all age groups.
Its incidence is rising as the number and use of available serotonergic drugs are increased in clinical practice.
Mechanism
Potential mechanisms include increased serotonin synthesis or release; reduced serotonin uptake or metabolism; and direct serotonin receptor activation. Addition of drugs that inhibit the cytochromes (e.g. CYP 2D6 and/or 3A4) to therapeutic regimens of selective serotonin reuptake inhibitors (SSRIs) could be another mechanism.
The majority of cases are iatrogenic from synergistic medication use, although cases of self-poisoning with serotonergic agents also occur.
Diagnosis
Diagnosis can be made using the Hunter Serotonin Toxicity Criteria:
Hunter’s rules for diagnosis of serotonin syndrome. (Ables AZ, Nagubilli R. Prevention, recognition, and management of serotonin syndrome. Am Fam Physician. 2010 May 1; 81(9):1139-42).
Symptoms can include anxiety, restlessness, confusion, sweating, muscle spasm or rigidity, rapid back and forth eye movement, shaking, fever, rapid heart rate, vomiting and diarrhea.
Symptoms can develop rapidly, within minutes of taking the drug, however, most patients present within couple of hours after a medication change or overdose.
Differential Diagnosis
The primary differential diagnosis of serotonin syndrome includes malignant hyperthermia, neuroleptic malignant syndrome, and anticholinergic syndrome. A complete history of the drugs or substances is helpful in ruling out these conditions. It is necessary to rule out initiation or change of dosage of dopaminergic drugs and other possibilities, such as infection, metabolic disorder, substance intoxication, or withdrawal. Other potential diagnoses include heat stroke, overdose of sympathomimetic drugs, delirium tremens, meningitis, encephalitis, thyroid storm, sepsis, or tetanus.
Treatment
First, Recognize the disease
Next, Stop the offending agent(s)
In the meantime, Supportive care (treat hyperthermia, autonomic dysfunction)
Benzodiazepines may be used to treat agitation and tremor.
Sometimes may administer serotonin antagonists, cyproheptadine or chlorpromazine.
Patients with moderate or severe cases of serotonin syndrome require hospitalization.
Critically ill patients may require neuromuscular paralysis, sedation, and intubation.
Prognosis
If serotonin syndrome is recognized and complications are managed appropriately, the prognosis is favorable. The severity of the disease can range from mild to life-threatening situation. However, most cases are mild and do not require hospitalization and generally resolve within 1 to 3 days by withdrawal of the offending agent and supportive care. Patients with moderate and severe cases may require hospitalization.
Prevention
Awareness of physicians and patients of the potential for toxicity from serotonergic drugs.
Always tell any doctor who prescribes you about all medications, herbal products and street drug you take.
When starting new medicine, have the pharmacist check for drug interaction
Avoiding the combined use of serotonin-augmenting drugs.
If you are already on medicine, do not take a new herbal or over-the-counter medicine without first checking with your doctor
Warning
If you have any symptoms of serotonin syndrome, please call your primary care physician and inform him/her of your suspicion before taking any steps.


































 His brain showed the same pathologic changes as the Punch Drunk boxers.
His brain showed the same pathologic changes as the Punch Drunk boxers.







