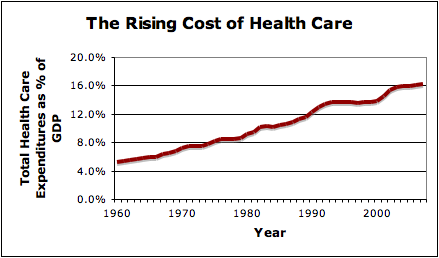
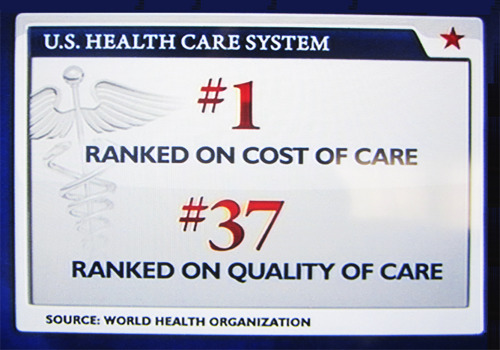
It’s no secret that health care costs are escalating.
Although physicians value their independence, part of the problem here is the unregulated use of costly tests, medications and procedures, many of which are unproven and of questionable benefit.
xx
Evidence based medicine assess the strength of the evidence of risks and benefits of treatments (including lack of treatment) and diagnostic tests in an attempt to help clinicians predict whether a treatment will do more good than harm.
However, less than 1 in 5 medical decisions in the USA are made based on evidence-based medicine.
xx

The American Academy of Neurology has recently taken a step in the right direction by publishing a list of 5 costly neurology practices which continue to be widely performed despite being of little proven benefit:
xx
1. Don’t perform electroencephalography (EEG) for headaches.
xx
2. Don’t perform imaging of the carotid arteries for simple syncope without other neurologic symptoms.
Syncope is caused by global cerebral hypoperfusion, not carotid artery disease, so even if a carotid stenosis is identified, it would be asymptomatic (see point number 5)
xx
3. Don’t use opioid or butalbital treatment for migraine except as a last resort.
Butalbital is effective short term treatment for migraine, but commonly leads to rebound, which ultimately exacerbates migraine. Click here for more information about migraine.
xx
4. Don’t prescribe interferon-β or glatiramer acetate to patients with disability from progressive, nonrelapsing forms of MS.
Interferon-β and glatiramer acetate, are effective for relapsing phases of MS, but do not prevent the development of permanent disability in progressive forms of multiple sclerosis. These medications cost more than $40,000 a year, and put a financial strain on the patients and their families to make the co-pays. In some series as many as 10%-15% MS patients have progressive forms of the disease and yet are still taking one of these medications.
xx
5. Don’t recommend carotid endarterectomy (CEA) for all patients with asymptomatic carotid stenosis.
Surgery is of much less benefit for asymptomatic carotid stenosis, and should be reserved for those with a perioperative complication risk of less than 3% and a life expectancy of greater than 3 to 5 years. Click here for more information about surgery for carotid artery disease.
xx
Click here for more details.
