Posted by Sara Ghotb, MD PGYIII Internal Medicine, Monmouth Medical Center
Case history:
This 74 y/o African American male presented to the emergency department with a 1-week history nausea ad intractable vomiting.
His past medical history included surgery for esophageal cancer in 2012 and hypertension.
He was admitted to the hospital for a gastrointestinal evaluation. His symptoms did not improve with antiemetics and he also began to complain of headache and dizziness. He was scheduled for an upper GI endoscopy.
Debra Haining lay in a hospital bed at Massachusetts General Hospital, awaiting surgery. Both eyelids were colored purple, and blue dots were drawn on her forehead, including one on each temple, and one above her left eye.
The dots indicated the location where she feels the migraine, the trigger points, where the pain strikes. She is 57 years old and says that she never had a headache until five years ago, when she woke up feeling as if she’d been shot through the head.
She was forced to spend nearly every day in bed with the curtains drawn. She could not tolerate light, smell, or sound. Typically she rose only to see her 12-year-old son off to school in the morning and in the afternoon when he returned. Until recently, she had an ice pack to her head and could not drive a car.
A half-dozen medications, four different pain clinics, a variety of headache cocktails and injections, and numerous neurologists didn’t provide relief. Haining, who lives in Pawtucket, R.I., searched the Internet until she found Dr. W.G. (Jay) Austen Jr., of plastic and reconstructive surgery at Massachusetts General Hospital.
Haining says she was tired of doctors who suggested that she learn to accept a lifetime of pain, pills, and shots, and was relieved to find a doctor who offered to treat the cause of the migraine and not just the symptoms. “When you are debilitated and life comes to a halt, you are willing to try what’s out there.’’
In the operating room at Mass. General, Austen began surgery on Haining by making an incision in one of her eyelids in what would appear to be a routine blepharoplasty, a cosmetic surgery known as an “eyelid lift.”
Haining would benefit cosmetically by removal of this globular flat that settles into each eyelid with age. But the point, Austen says, is that this particular procedure provides “easy access” to the critical sensory nerves around her eyes that he believes were causing migraine pain.
This was just one of the three trigger points that Haining identified prior to surgery, and as he operated, Austen would be seeking a structural reason for that pain, a nerve compressed or impinged by surrounding bone or soft tissue.
This surgical approach was developed 12 years ago by Dr. Bahman Guyuron, chairman of the plastic surgery department at University Hospitals Case Medical Center in Cleveland, after several of his plastic surgery patients reported that their migraines improved after a cosmetic procedure known as a forehead lift.
A study published in the journal Plastic and Reconstructive Surgery in 2009 — led by Guyuron and submitted by Case Western Reserve University, the American Migraine Center, and the Center for Headache and Pain, Cleveland Clinic — found that just under 85 percent of patients who underwent the nerve decompression surgery reported at least a 50 percent reduction in migraine, calculating pain, frequency, and duration. Nearly 60 percent (28 of 49 patients) reported a complete elimination of pain. This compared with only 1 of 26 patients who had a sham surgery, in which the surgery was limited to exposure of the nerve but muscle and attachments were left intact. Reported side effects included forehead numbness, temporary hair loss and itching, a slight hollowing of the temple, and small change in eyebrow movement.
In his recently published review on the subject, Dr Mathew explains that these surgeries are unproven, risky, expensive ($10,000-15,000) and are often not covered by medical insurance. “Many patients have no or temporary benefits from the surgery and still wind up on long term narcotics”, he says, and furthermore “These procedures have made their way into mainstream medicine without adequate investigation”. This is why he has decided to make this subject the focus of his future advocacy efforts.
However, the syndrome was unknown in the first manned space flights – none of the 26 astronauts who flew in the 16 Mercury and Gemini space trips experienced disorientation or motion sickness.
However, this changed with the Apollo missions, where there were 11 incidents of inflight motion sickness, ranging from mild to severe, in as many flight missions. This was attributed to the increased opportunity for movement by the crewmen within the relatively large volume of the combined Apollo command and lunar modules compared to the very confined crew compartments of the Mercury and Gemini spacecraft.
The problem got even worse with Skylab, where 5 of 9 astronauts experienced symptoms of motion sickness during the initial days of the flight, 2of them severe including vomiting.
Anti-motion sickness drugs used by the Skylab 3 and 4 crewmen were not completely effective in ameliorating symptoms.
Interestingly, these symptoms of motion sickness were temporary, and all resolved within a few days.
In fact, in-flight experiments conducted on or after day 8 showed that all crewmen had adapted to weightlessness, and did not experience any adverse symptoms in a spinning chair (30 rpm) sufficient to cause vertigo on Earth.
Maintaining an awareness of the relative location of our body parts requires the precise integration of visual, vestibular, and proprioceptive (touch, pressure, and stretch receptors in our skin, muscles, and joints) sensory inputs.
If your head moves in space, your eyes see the movement, but in zero-gravity the vestibular otolith doesn’t move and there is no proprioceptive input from the feet against the floor.
Space sickness is felt to be the result of “sensory conflict” or sensory mismatch.
It didn’t occur in the early Mercury and Gemini flights, because the astronauts spent the whole flight strapped into a seat inside a small capsule with limited opportunity for movement and minimal exposure to conflicting visual, motor, and vestibular sensory messages.
However, space sickness has affected >50% of astronauts since Apollo, beginning within the first hour of transition from Earth gravity to microgravity, and persisting for 2 to 3 days. It’s so predictable that no space walks were scheduled for the first 3-days of any Space Shuttle missions.
Recent research has suggested that virtual reality training can simulate specific effects of microgravity and may prove to be an effective countermeasure against space motion sickness through a process of habituation.
xx
Space Headache
Space flights can also trigger headaches. In a 2009 study 71% of astronauts reported headaches – occurring during launch, flight, activities outside the space station and landing. None had a history of recurrent headache on earth. There was little to no association with the main symptoms of space motion sickness, such as nausea, vomiting or vertigo.
Asked to describe the headache, the astronauts mostly said the symptoms were “exploding” or “heavy feeling.”
We know that blood volume gets redistributed to the brain and upper body when the astronaut floats in zero gravity.
This shift of blood towards the brain causes a painful increase in pressure within the skull:
Posted by Sonia Jasuja, MSIV Drexel University College of Medicine
As a current student of traditional Western Medicine, I have been trained to turn towards modern pharmacology and away from natural remedies, for the most part. However, as someone who has suffered from severe skin allergies all my life, I know how desperate patients can get in order to find something that really works! When Western Medicine fails us, where can we turn?
What is it? Butterber is an herbal plant that has been used for medicinal purposes, including migraine and headache, allergies, asthma, and many more. Most herbal remedies use the root extract in the form of a pill. It has properties that relieve spasms and decrease inflammation.1
Is it safe? Yes- studies have determined that Petasites is safe to use for the prophylaxis of migraine. The dose that was cited to have moderate efficacy is 150mg daily.2
Side effects are very mild and include burping, stomach upset, diarrhea, fatigue and itching.3
One important thing to keep in mind- make sure to only buy Petasites hybridus that is certified and labeled, “PA free”. “PA” stands for pyrrolizidine alkaloids, which cause adverse effects in the liver, lungs and circulatory system. PA’s can cause cancer.3
You should not take Petasites if you are pregnant or breast-feeding, have liver disease, or if you are allergic to ragweed, marigolds, daisies or other related herbs. 3
Does it work? Probably, but we still need more information! In 2006, Agosti et al. published “Effectiveness of Petasites hybridus preparations in the prophylaxis of migraine: A systematic review”. Of the two studies that were looked at, the systematic review showed that there is only moderate evidence for the effectiveness of Petasites at the dose of 150mg/day for a period of 3-4 months. The review also thoughtfully pointed out that confounding factors still need to be accounted for. These factors would include things like which migraine treatments have been successful or unsuccessful in the past, and any use of addictive or hormonal substances, such as nicotine or estrogens.2
The review article states that the overall effect size of the 150mg extract dose is approximately 15% percent lower migraine frequency rate per month compared to placebo.2
The bottom line. If you have frequent or debilitating headaches, you should see you doctor for an evaluation. You may need some diagnostic testing, and there are probably some very effective conventional medications you can try. However, if you are still having frequent headaches despite that, Petasites might be worth a try.
Case Summary:
This 46-year-old woman was healthy except for a history of occasional migraine headaches and cigarette smoking. On the day of admission she had fallen down a short flight of steps carrying a heavy box. About 2 hrs later she complained of some neck pain. Then later that evening developed abrupt onset left sided weakness. She arrived at the emergency room within 1.5 hrs of the onset of weakness. On examination, she was alert, but she had a right gaze deviation (she wouldn’t look to the left side) and the left side was completely paralyzed. She had a normal brain CT scan.
The stroke team was notified, and she was given intravenous thrombolytic (“clot busting”) drug therapy within 1/2 hr of her arrival at the hospital and 2 hrs since the onset of her symptoms.
In other cases, the specific cause of arterial weakness is unknown, but there is ongoing research to try to identify genetic links.
xx
What happens after a cervical artery dissection?
Symptoms can be caused from the damaged arterial wall itself (local symptoms) and some affected patients will later develop strokes.
Local symptoms include neck pain, unusual headache and/or Horner’s syndrome.
L Horner’s syndrome (small pupil and drooping eyelid) caused by damage to the sympathetic nerve fibers in the arterial wall from carotid dissection. Click here to find out more about Horner’s syndrome and other causes of unequal pupils.
xx
What about stroke?
Stroke symptoms only occur in 25-30% dissections and can occur several days after the neck trauma and/or onset of local symptoms.
The arterial dissection narrows the space inside the blood vessel (the lumen), so less blood flow gets to the brain:
A carotid artery dissection with blood clot inside the arterial wall (left) leading to narrowing of the vessel lumen and less blood flow (right).
Cervical arterial dissections can also cause stroke when pieces of blood clot break off and move with the blood flow only to block small arteries further inside the brain (cerebral thromboembolism), or if the dissection tracks across (and blocks off) an arterial branch (see below):
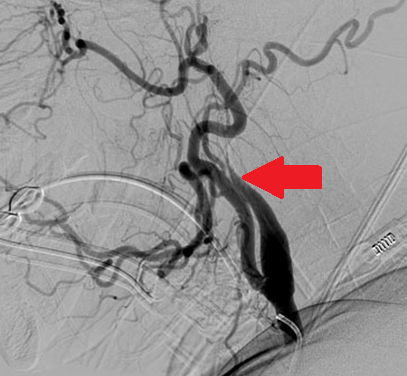
MR angiogram (left) showing tapered occlusion of the left internal carotid (white arrow) from dissection. Fat suppressed T1 weighted MR axial image through the dissected cervical artery (right) showing bright blood within it’s wall (black arrow) from dissection.
xx
How is it treated?
In most cases the arterial dissection ultimately heals on its own without any surgical intervention. There has been some controversy surrounding the use of anticoagulant vs anti-platelet drugs for stroke prevention after cervical artery dissection, but most current data favors the use of the anti-platelet drug aspirin:
Of course, for patients presenting with symptoms of acute stroke, throbolytic therapy is also an option, and can improve outcome without increased risk in stroke from dissection:
Click here to find out more about cervical artery and dissection and stroke.
Click here to find out what to do if you think your having a stroke.
Click here to find out more the certified stroke center at Monmouth Medical Center.
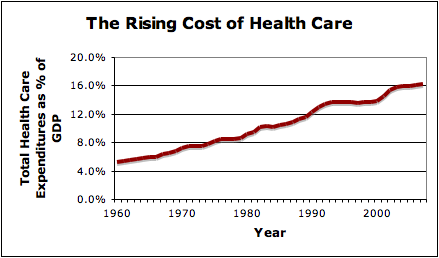
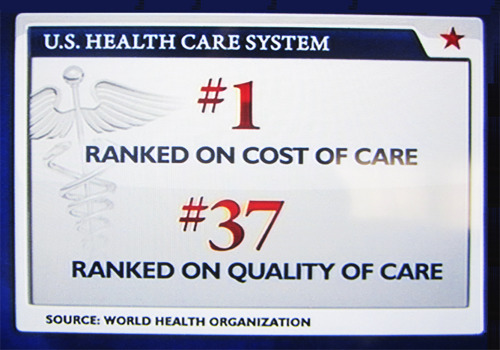
It’s no secret that health care costs are escalating.
Although physicians value their independence, part of the problem here is the unregulated use of costly tests, medications and procedures, many of which are unproven and of questionable benefit.
xx
Evidence based medicine assess the strength of the evidence of risks and benefits of treatments (including lack of treatment) and diagnostic tests in an attempt to help clinicians predict whether a treatment will do more good than harm.
However, less than 1 in 5 medical decisions in the USA are made based on evidence-based medicine.
xx
The American Academy of Neurology has recently taken a step in the right direction by publishing a list of 5 costly neurology practices which continue to be widely performed despite being of little proven benefit:
3. Don’t use opioid or butalbital treatment for migraine except as a last resort.
Butalbital is effective short term treatment for migraine, but commonly leads torebound, which ultimately exacerbates migraine. Click here for more information about migraine.
xx
4. Don’t prescribe interferon-β or glatiramer acetate to patients with disability from progressive, nonrelapsing forms of MS.
Interferon-β and glatiramer acetate, are effective for relapsing phases of MS, but do not prevent the development of permanent disability in progressive forms of multiple sclerosis. These medications cost more than $40,000 a year, and put a financial strain on the patients and their families to make the co-pays. In some series as many as 10%-15% MS patients have progressive forms of the disease and yet are still taking one of these medications.
Surgery is of much less benefit for asymptomatic carotid stenosis, and should be reserved for those with a perioperative complication risk of less than 3% and a life expectancy of greater than 3 to 5 years.Click here for more information about surgery for carotid artery disease.
Caused by a disturbance of perception rather than an actual physiological change
– Altered body image (Ex: big buildings look same size as person’s own body)
– Distorted perception of size (micropsia, macropsia)
– Distorted perception of the shape of objects – Loss of spatial perspective (sense of time and space)
– Auditory or tactile hallucinations
AIWS generally affects a younger population and has several associated conditions. Migraine is the classic diseaselinked to AIWS, the distorted sensations can either begin before a migraine (aura or “warning”) or afterwards, and in younger patients can even occur without headache
Certain tests & imaging studies helprule out secondary causes: – urine toxicology screen
– monospot test(for mononucleosis)
–MRI brain – with and without contrast (to look for malignancy)
– EEG(to detect seizures or seizure-like activity)
Sounds scary, right? Well, good news is it’s not as bad as it sounds. Most patients who experience AIWS as children will outgrow the condition as adults. Patients should be monitored for worsening of symptom severity and frequency. If all studies are negative and the patient continues to improve clinically, then further evaluation and/or treatment is not needed. Bestmanagement for future attacks is focused on migraine prophylaxisand lifestyle modifications (healthy diet, regular exercise, adequate sleep).
Posted By Sidra Ghafoor, Drexel University College of Medicine Class of 2013
2. Athletes who sustain a sports related concussion and require immediate medical attention will be evaluated in the Monmouth Medical Center Emergency Room. If they are felt to be suffering from ongoing symptoms of concussion, they can be referred to the Monmouth Concussion Center for same or next day evaluation by a neurologist and return to play determination.
4. The results of these evaluations with be forwarded to the athlete’s primary physician and athletic trainer, and arrangements will be made for appropriate follow-up.
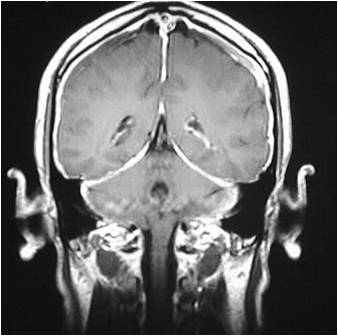
A 44-year-old man is sent to the ED directly from a radiology facility after a MRI brain showed “meningitis”.
The report says “….diffuse enhancement of the meninges, indicating an infectious or neoplastic meningitis”.
He has had a 2 week history of occipital headaches that get progressively worse during the day, and were relieved by laying down, with some associated neck pain and tinnitus.
His exam in normal, he has no fever and he doesn’t look sick.
Here’s the MRI:
Would you do a lumbar puncture? Why? What would you do?


























 Other causes of Alice in Wonderland Syndrome are:
Other causes of Alice in Wonderland Syndrome are: